








 India Cancer Surgery Site is one of the most prestigious and leading group of oncologists, cancer surgeons, and physicians dedicated to fight various different types and stages of cancer with the best medical facilities and infrastructure at a very affordable cost.
India Cancer Surgery Site is one of the most prestigious and leading group of oncologists, cancer surgeons, and physicians dedicated to fight various different types and stages of cancer with the best medical facilities and infrastructure at a very affordable cost.
Our group is involved and dedicated to deliver quality and low cost cancer treatment at best hospital in India to people from all over the world. Our association with the top cancer hospitals in the world offers the finest healthcare facilities to help the patients seeking medical care and specialty treatments from the best oncologist in India.
When we talk about cancer, the seriousness creates many trembling waves deep within our minds and hearts. At times, it comes to deep thinking that why do we actually need cancer treatment.
Researchers and statisticians have revealed the answers in their cancer statistics and global research reports: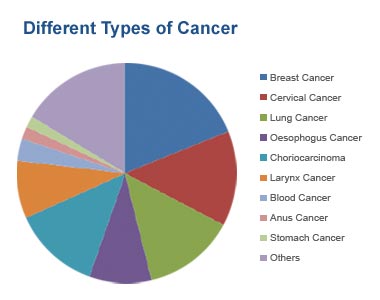
Moving alongside, we are here for you with a powerful group at India Cancer Surgery Site have a long list of best cancer surgeon in India filled with passion and dedication to win the tough battle that otherwise goes on fighting a lifetime.
Our thought process also includes practical and effective measures for making every cancer journey easier and successful with our forte:
 There is a very famous quote by Oprah Winfrey, "Know what sparks the light in you. Then use that light to illuminate the world."
There is a very famous quote by Oprah Winfrey, "Know what sparks the light in you. Then use that light to illuminate the world."
We have a team that gets their spark by treating those in pain and need and we are trying every day to light up the world around us a little bit by giving a painless life to every patient that comes to us for their cancer treatment.















With a normal earache, it had started. Mr.Lawrence Oluwadare, the civilian of Nigeria, did not notice at first. However, gradually some other signs started to become noticeable. He lost some weight and his voice changed a little. With a sore throat and trouble in swallowing even the saliva, he shared his problem with his wife Mrs.Faith Wisdom Oluwadare. They decided to show up to a doctor in their neighborhood. The riskiest matter was the blood in his cough. The consulting doctor there diagnosed Mr Oluwadare with neck cancer...... Read More
With a normal earache, it had started. Mr.Lawrence Oluwadare, the civilian of Nigeria, did not notice at first. However, gradually some other signs started to become noticeable. He lost some weight and his voice changed a little. With a sore throat and trouble in swallowing even the saliva, he shared his problem with his wife Mrs.Faith Wisdom Oluwadare. They decided to show up to a doctor in their neighborhood. The riskiest matter was the blood in his cough. The consulting doctor there diagnosed Mr Oluwadare with neck cancer. There was complete silence and both husband and wife were shattered to hear and accept the truth. However, truth cannot be hidden and has to be faced. His wife immediately got on her toes to search for a good cancer surgeon and in the process, she consulted many doctors and cancer specialists in Nigeria. Eventually, not to wait more as it could be more dangerous if not treated on time. However, she failed to gain a feeling of contentment in Nigeria with all respect.
Mr. Lawrence Oluwadare’s colleague acknowledged about India Cancer Surgery Group in India. Mrs. Oluwadare without any waste of time contacted them for their services. The first conversation was satisfactory and thereafter all the communications were falling so smoothly and to the package that the husband and wife could manage to shed out. This game them a sense of comfort and relief. Hence, they made up their mind to visit India for the surgery. India Cancer Surgery Group confirmed their arrival date and made all the arrangements for their travel and stay in India. On arrival, the expert and experienced team was all ready with the pickup and drop facility, accommodation booking, appointment, and other essential amenities. The visit to the best cancer surgeon in India was considerable and helpful. His persistent cough defined a lot about his misery. Moreover, the other symptoms shared with the doctor made him decide to scrutinize Mrs. Oluwadare deeply. For a deeper examination, physical examination was done through few combined tests that could determine the further treatment. The tests were blood and urine test, Endoscopy, Biopsy, Molecular testing of the tumor, X-ray/barium Swallow, Panoramic Radiography, ultrasound, Computed Tomography (CT or CAT) Scan, Magnetic Resonance Imaging (MRI), Bone Scan, and Positron Emission Tomography (PET) or PET-CT Scan.
During the physical examination and other pre-surgery process, the consulting cancer surgeon in India advised him to continue with his forgoing medications until the reports are clear and well inspected. The doctor inspected the reports and immediately altered his medicines for preoperational treatment. The doctor decided to operate as soon as possible and gave him the date in that coming week. It was a hard time for Mr. and Mrs. Oluwadare as they never imagined that a little earache and cough would result in a dangerous disease like cancer. Tough times are difficult to pass but they consoled each other. Certainly, their wait ended when the day arrived when the operation was scheduled. Mr. Oluwadare was beset by numerous feelings like anxiety, fear and felt goose bumps all over. The doctor ensured them in a positive way. Mrs. Oluwadare sat outside the operation theatre with all the mental pressure of anxiety and depression, yet showed signs of positivity. The team of the group further consoled her during the surgery and assured her of a successful operation. The doctor came outside and blissfully announced Mrs. Oluwadre’s name and informed him that the surgery ended well. The surgeon also mentioned that for the post-operational treatment, he needed to take precautions in his diet. They made him stay in the hospital for two days and on the third day, he got discharged. Mr. and Mrs. Oluwadare were overwhelmed with the generosity of the staff and the doctors who were on duty at that time. Their hospitality was highly perceptible!
Thank you,
Mr. Lawrence Oluwadare
Nigeria















